Introduction
This is a physician-facing reference for preparing patients for, and following them after, bariatric surgery in the Western Zone. It covers obesity classification and staging, surgical candidacy, pre-operative assessment and workup, peri-operative medication considerations, and the post-operative laboratory schedule for both sleeve gastrectomy and Roux-en-Y gastric bypass.
How to use this guide
A quick reference for primary care and referring clinicians — not a substitute for the bariatric program’s own protocols or for clinical judgement. All anti-obesity medications and the timing of their discontinuation should be reviewed with the surgical and anesthesia teams pre-operatively.
Section 1 · Pre-Operative Assessment
Classification & staging
A. Obesity classification (WHO / Obesity Canada)
| Class | BMI (kg/m²) |
|---|---|
| Class I | 30.0–34.9 |
| Class II | 35.0–39.9 |
| Class III | 40.0–49.9 |
| Class IV | 50.0–59.9 |
| Class V | ≥60.0 |
Enter weight and height (any units) to calculate BMI and obesity class automatically.
B. The 4 M’s framework
Assess each patient across all four domains prior to referral (Obesity Canada).
| Domain | Key considerations |
|---|---|
| Mental health | Depression, anxiety, PTSD, binge eating disorder (BED), emotional eating, body image, history of trauma/abuse. Screen with PHQ-9, GAD-7, and a BED screener (BEDS-7; see Section 1G). |
| Mechanical | OSA, OA, GERD, urinary incontinence, mobility limitations, chronic pain, functional impairment. |
| Metabolic | T2DM / insulin resistance, dyslipidemia, NAFLD/NASH, PCOS, HTN, metabolic syndrome. |
| Monetary / milieu | Socioeconomic barriers, food insecurity, access to follow-up, coverage for medications, support systems, cultural considerations. |
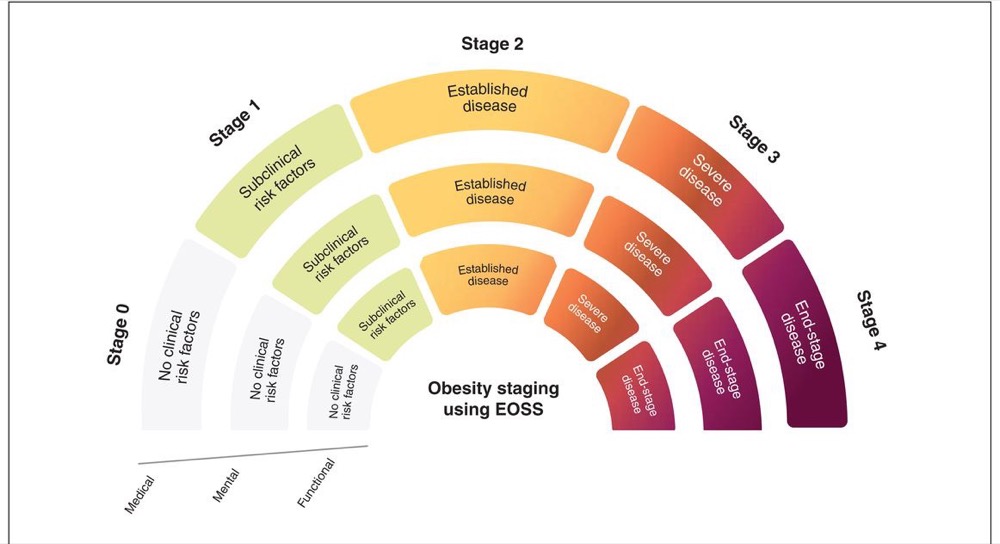
C. Edmonton Obesity Staging System (EOSS)
| Stage | Description |
|---|---|
| 0 | No obesity-related risk factors or symptoms |
| 1 | Subclinical risk factors (e.g., borderline HTN, impaired fasting glucose, elevated liver enzymes) |
| 2 | Established obesity-related chronic disease (T2DM, OSA, GERD, PCOS, HTN, dyslipidemia, OA) |
| 3 | End-organ damage (MI, heart failure, diabetic complications, disabling OA) |
| 4 | Severe / end-stage disability or life-threatening conditions |
Surgical candidacy is generally considered at EOSS Stage 2–3. Stage 4 may require careful risk–benefit analysis.
Section 1D
Surgical criteria & procedures
Indications for bariatric surgery (Obesity Canada guidelines):
- BMI ≥40 kg/m² (Class III), or
- BMI ≥35 kg/m² (Class II) with at least one obesity-related comorbidity (T2DM, OSA, HTN, NAFLD, GERD, dyslipidemia, PCOS, OA), or
- BMI 30–34.9 kg/m² with poorly controlled T2DM (case-by-case)
| Procedure | Mechanism | Key considerations |
|---|---|---|
| Sleeve gastrectomy (VSG) | Restrictive; ~80% of stomach removed | Lower malabsorption risk; may worsen GERD; simpler anatomy |
| Roux-en-Y (RYGB) | Restrictive + malabsorptive | Better for GERD and T2DM; higher micronutrient deficiency risk; dumping syndrome possible |
Section 1E
Medications to consider pre-operatively
| Medication | Notes |
|---|---|
| Liraglutide (Saxenda) 3.0 mg SC daily | GLP-1 RA; may assist with pre-op weight loss; stop on day of surgery |
| Semaglutide (Wegovy) 2.4 mg SC weekly | GLP-1 RA; superior weight-loss efficacy; stop 2–4 weeks pre-op per anesthesia/surgical guidance |
| Naltrexone/bupropion (Contrave) | Useful with concurrent depression/cravings; CI in seizure disorder, opioid use, uncontrolled HTN |
| Orlistat (Xenical) | May assist modestly; GI side effects; rarely used pre-operatively |
| Topiramate (off-label) | May reduce BED behaviours; CI in pregnancy; monitor for cognitive side effects |
| Metformin | Continue if T2DM / insulin resistance; adjust post-op as glucose improves |
⚠ Concerns & contraindications
GLP-1 RAs — risk of aspiration from delayed gastric emptying; discuss timing of discontinuation with anesthesia. Contrave — avoid with seizure history, bulimia, or opioid use. All anti-obesity medications should be reviewed by the surgical team pre-operatively.
Section 1F
Pre-operative workup
Routine bloodwork
- CBC, electrolytes, Cr, eGFR, fasting glucose, HbA1c
- Lipid panel (TC, LDL, HDL, TG)
- Liver panel (AST, ALT, ALP, GGT, bilirubin, albumin)
- TSH
- Iron studies (ferritin, serum iron, TIBC, transferrin saturation)
- Vitamin B12, folate, 25-OH vitamin D, calcium, PTH
- Vitamin A, vitamin E, zinc, copper (especially if RYGB planned)
- INR/PT if liver disease suspected
- Fasting insulin (optional, if assessing insulin resistance)
- HBsAg, anti-HCV, HIV (per institutional protocol)
EGD (esophagogastroduodenoscopy)
- Recommended pre-operatively, particularly if RYGB planned (stomach becomes inaccessible post-op)
- Assess for Barrett’s esophagus, hiatal hernia, ulcers, gastritis, H. pylori
- Biopsy for H. pylori — if positive, treat and confirm clearance before surgery
H. pylori testing
- Test all patients pre-operatively (serology, stool antigen, or biopsy via EGD)
- If positive: eradication therapy (e.g., PPI + clarithromycin + amoxicillin × 14 days, or bismuth quadruple therapy)
- Confirm eradication with urea breath test or stool antigen ≥4 weeks after treatment
Additional investigations
- ECG (baseline, especially with cardiac risk factors)
- Sleep study / polysomnography if OSA suspected — initiate CPAP pre-op if positive
- Abdominal ultrasound (cholelithiasis, NAFLD assessment)
- Chest X-ray (per anesthesia requirements)
- DEXA scan if osteoporosis risk factors present
Section 1G
Binge eating disorder (BED) screening
Screen all candidates for BED prior to referral. Untreated BED is associated with poorer surgical outcomes and higher risk of weight regain.
Screening tools
- BEDS-7 (Binge Eating Disorder Screener-7) — brief, self-report; a positive screen warrants further assessment
- Binge Eating Scale (BES) — score ≥17 suggests moderate BED; ≥27 severe
- LOCES-Brief (Loss of Control over Eating Scale, 7-item) — validated in bariatric populations; predicts post-operative eating outcomes
- QEWP-5 (Questionnaire on Eating and Weight Patterns-5)
- Clinical interview: frequency of binge episodes, loss of control, distress, compensatory behaviours
If BED identified
- Refer to psychiatry/psychology with eating-disorder expertise
- Consider CBT, DBT, or interpersonal therapy pre-operatively
- Pharmacotherapy: lisdexamfetamine (Vyvanse) — Health Canada approved for moderate–severe BED; topiramate (off-label); SSRIs for comorbid depression
- BED does not necessarily preclude surgery, but should be stabilized pre-operatively
- Consider GLP-1 or GIP/GLP-1 therapy for other obesity complications and monitor BED symptoms
- BED may resolve after surgery, or may arise post-operatively in those without prior history
Section 1H–I
Cancer screening & NSAID avoidance
H. Routine cancer screening (ensure up to date)
| Screening | Guideline |
|---|---|
| Pap smear | Per provincial guidelines (q3yr ages 25–69, or as indicated) |
| Mammogram | Ages 40/50–74 per provincial guidelines; q1–2yr |
| Colonoscopy | Age ≥50 (or ≥45 if high risk); q10yr if average risk |
| FOBT / FIT | q1–2yr if not undergoing colonoscopy |
| Iron studies | Baseline mandatory — rule out occult GI malignancy if iron deficiency present pre-operatively |
Post-surgical anatomy (especially RYGB) may limit future endoscopic evaluation — complete all age-appropriate cancer screening prior to surgery.
I. NSAID avoidance
⚠ NSAIDs are permanently contraindicated post-operatively
Risk of marginal ulcers, anastomotic ulcers, perforation, and GI bleeding (especially post-RYGB). Discontinue all NSAIDs (ibuprofen, naproxen, ASA, diclofenac, celecoxib) pre-operatively. Alternatives: acetaminophen, tramadol, topical analgesics, PPI for gastroprotection. Update the medication list / allergy alerts in the chart.
Section 1J–L
Lifestyle, mental health & dietitian referral
J. Smoking & alcohol cessation
Smoking
- Complete cessation required minimum 3–6 months pre-operatively; confirm with urine cotinine if needed
- Smoking increases risk of anastomotic leak, marginal ulcers, DVT/PE, and impaired wound healing
- Offer NRT, varenicline (Champix), bupropion, and cessation counselling
Alcohol
- Screen with AUDIT-C or CAGE
- Post-bariatric patients are at increased risk of AUD due to altered metabolism (faster absorption, higher peak BAC, reduced first-pass metabolism — especially post-RYGB)
- If current AUD or heavy use: refer for addiction support; surgery may be deferred until stable sobriety is demonstrated
- Counsel on lifelong moderation/abstinence post-operatively
K. Mental health assessment
- Screen with PHQ-9 (depression) and GAD-7 (anxiety)
- Assess for PTSD, trauma history, self-harm, suicidality; evaluate relationship with food, emotional eating, night eating syndrome
- Ensure realistic expectations regarding surgical outcomes; psychiatric/psychological clearance per program protocol
- Stabilize active untreated psychiatric illness before proceeding
- Post-bariatric patients have elevated suicide risk — ensure ongoing mental health follow-up
L. Dietitian referral
- Refer to a registered dietitian (RD) with bariatric expertise at the time of surgical referral — use the Western Zone Care Map to find local dietitian availability
- Pre-operative RD assessment: nutritional status, eating patterns, food security, disordered eating, supplement review
- Pre-operative diet education: total meal replacement (TMR) protocol, post-op dietary stages (clear → full liquids → pureed → soft → regular)
- Review the WZON Nutrition Guide for Bariatric Surgery with the patient
- Post-operative RD follow-up recommended at 4 weeks, 8 weeks, and 6 months
Section 2 · Post-Operative Follow-Up Labs
Post-operative laboratory schedule
A. Post–sleeve gastrectomy (SG)
| Timing | Labs |
|---|---|
| 3 months | CBC, electrolytes, Cr, fasting glucose, HbA1c, lipid panel, liver panel, ferritin, iron studies, B12, folate, 25-OH vitamin D, calcium, PTH, albumin |
| 6 months | Repeat above |
| 12 months | Repeat above + vitamin A, zinc, copper if clinically indicated |
| Annually | CBC, ferritin, iron studies, B12, folate, 25-OH vitamin D, calcium, PTH, HbA1c, lipid panel, liver panel, albumin |
B. Post–Roux-en-Y gastric bypass (RYGB)
| Timing | Labs |
|---|---|
| 3 months | CBC, electrolytes, Cr, fasting glucose, HbA1c, lipid panel, liver panel, ferritin, iron studies, B12, folate, 25-OH vitamin D, calcium, PTH, albumin, vitamin A, vitamin E, zinc, copper, thiamine (B1) |
| 6 months | Repeat above |
| 12 months | Repeat above + DEXA scan if osteoporosis risk |
| Annually | CBC, ferritin, iron studies, B12, folate, 25-OH vitamin D, calcium, PTH, vitamin A, vitamin E, zinc, copper, thiamine (B1), HbA1c, lipid panel, liver panel, albumin, INR if on anticoagulation |
⚠ RYGB-specific
Higher risk of fat-soluble vitamin (A, D, E, K), B12, and iron deficiencies, calcium malabsorption, and thiamine deficiency. Thiamine (B1) deficiency is a medical emergency — suspect in patients with persistent vomiting, neuropathy, or encephalopathy (Wernicke’s).
C. Key post-operative reminders
- NSAIDs — permanently contraindicated
- Alcohol — strongly discourage; altered metabolism increases AUD risk
- Smoking — lifelong cessation; ongoing ulcer and complication risk
- Mental health — ongoing monitoring; elevated suicide risk; ensure continued follow-up
- Pregnancy — avoid for 12–18 months post-op; ensure reliable contraception; monitor nutrition closely if pregnancy occurs
- Dumping syndrome (RYGB) — educate on avoiding high-sugar/high-fat meals
- Supplements — lifelong bariatric multivitamin + calcium citrate + vitamin D + B12 (sublingual or IM if malabsorptive) + iron as needed
- Dietitian follow-up — RD at 4 weeks, 8 weeks, 6 months, and as needed thereafter
Pre-Operative Checklist
Bariatric surgery pre-operative checklist
A working checklist for the initial evaluation and preparation phases. See the sections above for detail.
Classification & assessment see Sections 1A–C ›
Complete the BMI calculator, the 4 M’s, and select an EOSS stage in Sections 1A–C. The results carry down to the assessment summary at the end of this checklist.
Mental health considerations see Section 1K ›
Referrals to consider see Sections 1K–L ›
Dietitian & nutrition see Section 1L ›
Lifestyle & cessation see Section 1J ›
Initial bloodwork see Section 1F ›
Investigations see Section 1F ›
Follow-up schedule (months) see Section 2 ›
- Family doctor: 1, 3, 6, 12
- Dietitian: 1, 2, 6, 12 (plus 1 week post-op)
- Surgeon: 1, 6, 12
- Consider: psychology, kinesiology, other allied-health support
Assessment summary
Read-only — auto-filled from the BMI calculator and EOSS selector in Section 1.