Welcome
If you are reading this guide, you or someone you love may be thinking about bariatric surgery. This is an important step, and we are here to help you understand your options.
The most important thing to know is this: struggling with your weight is not your fault. Obesity is a medical condition, not a choice. Your body has powerful systems that control hunger, cravings, and how it stores fat. These systems can make managing weight very hard, no matter how hard you try.
Key message
Bariatric surgery is not “taking the easy way out.” It is a real medical treatment for a real medical condition. It changes your body’s biology to help you lose weight and improve your health.
This guide will give you the knowledge you need to make an informed decision. Understanding the science of obesity and how surgery works is the first step toward long-term success.
About the Network
About the Western Zone Obesity Network
The Western Zone Obesity Network (WZON) was created to improve obesity care in Nova Scotia. We bring together patients, doctors, nurses, dietitians, and other healthcare providers to give you the best possible care.
Our team & surgeons
- Medical Lead: Dr. Michael Mindrum
- Surgical Lead: Dr. Victoria Bentley
- Dietitian Lead: Kate Wentzell, RD
- Bariatric Surgeons: Dr. Ryan Kelly, Dr. Victoria Bentley
How we work together
Your care will involve a team that may include:
- Your family doctor or nurse practitioner
- A dietitian to help with nutrition
- A psychologist or counsellor for mental health support
- A kinesiologist or exercise specialist
- Internal medicine specialists (for complex medical conditions)
- Your bariatric surgeon
We believe the best care happens close to home. Your family doctor will be your main point of contact throughout your journey.
How It Works
Understanding bariatric surgery
More than just a smaller stomach
Many people think bariatric surgery just makes your stomach smaller so you eat less. But it does much more than that. Bariatric surgery is really a “metabolic” treatment – it changes how your body and brain communicate about hunger, fullness, and energy.
How it works
- Hunger hormones decrease. The part of your stomach that makes the “hunger hormone” (ghrelin) is removed or bypassed. This means you feel less hungry overall.
- Fullness hormones increase. Surgery changes how food moves through your digestive system. This leads to higher levels of hormones that tell your brain you are full and satisfied.
- Your brain’s “set point” changes. Your brain has a “thermostat” for body weight. Surgery helps reset this thermostat to a lower level, making it easier for your body to stay at a lower weight.
- Blood sugar improves. Changes in gut hormones help your body use insulin better. This is why many people with type 2 diabetes see major improvements – sometimes even going into remission.
The bottom line
Bariatric surgery works WITH your biology instead of against it. It changes the automatic, unconscious systems that drive hunger and weight gain.
Types of Surgery
Types of bariatric surgery
The Western Zone offers two types of bariatric surgery. Both are done using “laparoscopic” (keyhole) surgery through small incisions.
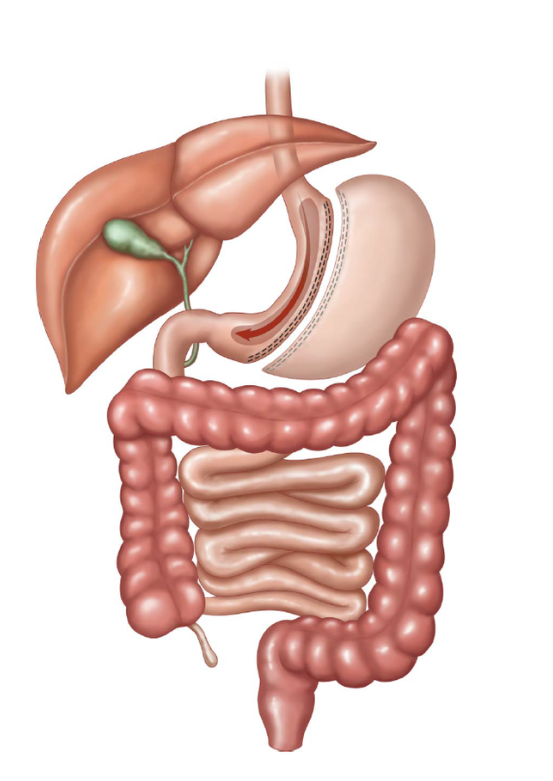
1. Vertical Sleeve Gastrectomy (VSG)
“Gastric sleeve” or just “the sleeve”
The procedure: the surgeon removes about 80% of the stomach, leaving behind a thin, banana-shaped stomach.
How it helps you lose weight
- Smaller stomach – you feel full after eating much smaller amounts
- Less hunger hormone – the removed part makes most of your ghrelin, so you feel less hungry
- Hormonal changes – other gut hormones shift to help your brain recognize fullness
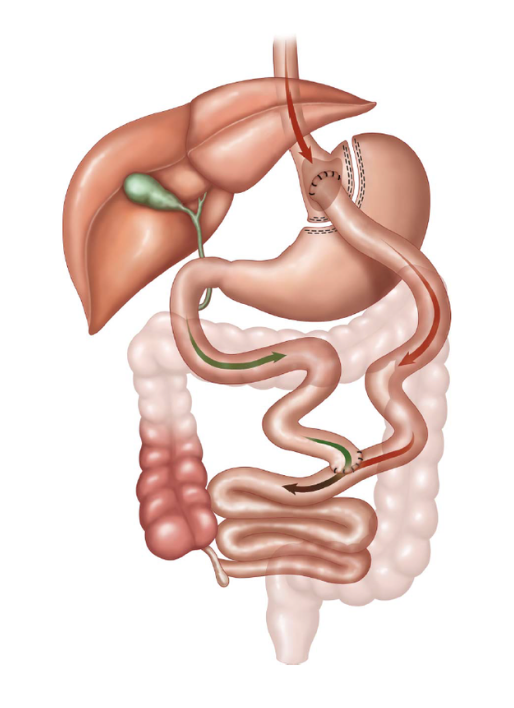
2. Roux-en-Y Gastric Bypass (RYGB)
“Gastric bypass”
The procedure: the surgeon creates a small pouch (about the size of an egg) from the top of your stomach. Then the small intestine is cut and reconnected in a “Y” shape, so food bypasses most of your stomach and the first part of your intestine.
How it helps you lose weight
- Very small stomach pouch – you can only eat small amounts at a time
- Less calorie absorption – your body absorbs fewer calories from food
- Major hormonal changes – powerful changes to gut hormones that control hunger and blood sugar
Bypass surgery may be recommended if you have:
- Severe acid reflux (GERD) that has not responded to other treatments
- Type 2 diabetes that needs better control
- Had a sleeve gastrectomy before but regained weight
Comparing the two surgeries
| Sleeve Gastrectomy | Gastric Bypass (RYGB) | |
|---|---|---|
| The surgery | 80% of stomach removed, leaving a banana-shaped sleeve; irreversible | Small pouch created, intestine rerouted in a Y-shape; potentially reversible |
| Average weight loss | 20–25% of total body weight | 25–30% of total body weight |
| Surgery time | About 1 hour | About 1.5–2 hours |
| Vitamin needs | Daily multivitamin, B12, vitamin D, calcium | More supplements needed due to less absorption |
| Best for | Most patients; simpler procedure. Patients who need NSAIDs, prior surgeries, higher starting weight, patients with IBD or cirrhosis | Severe diabetes and metabolic disease, severe acid reflux (GERD) |
| Complications in the first 30 days | Death, leak, bleeding, infection, blood clot | Death, leak, bleeding, infection, blood clot |
Comparing the two surgeries: late complications
| Late complication | Sleeve | Bypass |
|---|---|---|
| Anastomotic ulcer | — | + + |
| Stenosis / narrowing | + | + |
| Incisional hernia | + | + |
| Internal hernia | — | + |
| Gallstones and kidney stones | + | + |
| Dumping syndrome | — | + |
| Vitamin deficiency and malnutrition | + | + + |
| Chronic abdominal pain | + | + + |
| Low blood sugars | + | + + |
| Nausea / vomiting | + | + |
Your surgeon will recommend the best option for you based on your health conditions, not just which one has more weight loss.
Eligibility
Who can have bariatric surgery?
To be considered for bariatric surgery in Nova Scotia, you must meet certain requirements:
Weight requirements (at least one)
- BMI of 40 or higher, OR
- BMI of 35 or higher WITH a serious health condition related to weight (such as type 2 diabetes, sleep apnea, or heart disease), OR
- BMI of 30–35 WITH type 2 diabetes that is hard to control despite your best efforts
Other requirements
- No strict age limit – your team will assess your individual situation, but mortality is higher for patients of advanced age
- No strict upper weight limit, but special assessment is needed for BMI over 60
⚠ Important: smoking and cannabis
You MUST be smoke-free (no cigarettes, vaping, or cannabis) for at least 6 months before surgery. This is a safety requirement, not optional. Smoking greatly increases your risk of serious complications.
Surgery may not be right for you if:
- You are currently smoking or using cannabis
- You have current problems with alcohol or drug use
- You have an untreated eating disorder (like binge eating or bulimia)
- You have severe mental health problems that are not stable
- You have medical conditions that make surgery too risky
✓ Is there a cost?
Good news! Bariatric surgery is covered by the Nova Scotia provincial health plan. You do not have to pay for the surgery itself, but you will need to be able to pay for meal replacement pre-operatively and multivitamins lifelong.
Benefits & Risks
Benefits and risks of surgery
Potential benefits
Major health improvements
- Type 2 diabetes – many patients see major improvement or complete remission
- High blood pressure – often improves or goes away completely
- Sleep apnea – improvement or resolution of OSA
- High cholesterol – usually improves significantly
- Joint pain – less pain due to less weight on joints
Quality-of-life improvements
- More energy for daily activities
- Better mobility and ability to exercise
- Improved mood and mental health
- Better sleep
- Longer life expectancy
Potential risks
Like any major surgery, bariatric surgery has risks. It is important to understand short-term risks (within 30 days of surgery):
| Complication | How often |
|---|---|
| Bleeding | 1–5 in 100 patients |
| Leak from surgical connection | 1–3 in 100 patients |
| Blood clot in legs | 1–2 in 100 patients |
| Blood clot in lungs | About 1 in 200 patients |
| Death from surgery | Less than 1 in 100–1000 patients |
The overall chance of having ANY complication is about 10%. Most complications can be treated successfully.
Long-term considerations
- Gallstones – rapid weight loss can cause gallstones to form and become symptomatic.
- Nutritional deficiencies – you will need to take vitamins and minerals for life.
- Marginal ulcers – a sore that forms where the stomach pouch meets the small intestine after a RYGB; the main cause is smoking, NSAID use, or tension during surgery.
- Internal hernia – happens when the intestines shift into gaps created during surgery, occurring in about 1% to 5% of cases and often triggered by significant weight loss. If you have abdominal pain after a RYGB, seek medical attention.
- Increased risk of alcoholism and addiction in some.
- Dumping syndrome (diarrhea, flushing, fast heart rate) occurs in 50% or more cases at some point after a RYGB, and in 10 to 15% of patients after a VSG.
- Low blood sugars can occur in up to 20% of people after meals with RYGB, and less frequently in VSG. Severe symptoms requiring hospitalization are rare.
Weighing the decision
For most patients, the health risks of living with severe obesity are greater than the risks of surgery. Your healthcare team will help you understand your personal risk level.
What to Expect
What results can you expect?
Realistic weight-loss expectations
Here is what studies show about weight loss after surgery:
Sleeve gastrectomy
- Average: 20–25% of total body weight lost
- 300 lb person → expect to reach about 225–240 lbs
- 250 lb person → expect to reach about 187–200 lbs
Gastric bypass
- Average: 25–30% of total body weight lost
- 300 lb person → expect to reach about 210–225 lbs
- 250 lb person → expect to reach about 175–187 lbs
Understanding the numbers
These are averages. Some people lose more, some lose less. Your results depend on many things: your genes, your age, your starting weight, your hormones, and how well you follow the program. Results that are different from average are not a “failure” – they are your biology.
The true goal: better health
The goal of bariatric surgery is to improve your health – not to reach a specific number on the scale. Many patients will still be in the “obese” category by BMI after surgery. But they often have improvements in their health, mobility, function, energy, quality of life, and work productivity.
This is success! Health improvements matter more than any number on a scale.
Getting Ready
Getting ready for surgery
Preparing for bariatric surgery takes time and effort. This preparation is important for two reasons:
- It makes the surgery safer
- It builds the skills you need for long-term success
How to get a referral
- Learn about the program: read this guide and visit valleymetabolichealth.com
- Talk to your doctor: your family doctor, nurse practitioner, or specialist can send a referral to our surgeons
- Work with your team: you will work with dietitians, counsellors, and others to get ready
Surgery readiness checklist
Knowledge and understanding
- Understand obesity as a medical condition
- Understand the risks and benefits of surgery
- Have realistic expectations for weight loss
- Know what life will be like after surgery
Nutrition
- Work with a dietitian
- Understand the post-surgery diet stages
- Know how to get enough protein
- Reduce ultra-processed foods
- Take recommended supplements
- Read the companion Nutrition Guide for Bariatric Surgery
Lifestyle
- Smoke-free and cannabis-free for at least 6 months
- Regular physical activity in your routine
- Work on behaviour change with a counsellor if needed
Medical
- Have an established primary care clinician
- Blood work completed
- Sleep apnea test completed (and using CPAP if needed)
- Mental health stable and supported
- Cancer screening up to date
- Other medical conditions assessed
- Consider the impact of surgery on your medications
- Avoid NSAIDs (Motrin, ibuprofen, Advil)
Support
- Have a support person to help during recovery
- Plan for follow-up appointments
After Surgery
After surgery: the first few weeks
In the hospital (1–2 days)
Most patients stay in the hospital for 1–2 nights. During this time:
- You will start sipping clear fluids
- You will be encouraged to walk the same day as surgery
- Pain will be managed with medication
- You will be monitored for any early complications
At home: what to expect
The first 4–6 weeks at home are for healing. Here is what is normal:
Energy
- Feeling tired and weak is normal
- You may need frequent rest and naps
- Simple tasks may feel hard at first – this gets better over time
Activity
- Walk as much as you can – this helps prevent blood clots
- Do NOT lift anything heavier than 10–15 pounds for 6 weeks
- Do NOT drive while taking prescription pain medication
Incision care
- You can shower 48 hours after surgery
- Pat incisions dry gently
- Leave white strips (Steri-Strips) in place – they fall off on their own or can be removed at post-operative day 7–10
- No baths or swimming until incisions are fully healed (2–3 weeks)
Pain medication
- Take medications as prescribed
- For sleeves: take naproxen every 2 hours for 3 days
- For RYGB: take acetaminophen (Tylenol) for pain every 6 hours for 3 days, NO NSAIDs (aspirin, ibuprofen (Advil), and naproxen (Aleve))
Stomach pill
- You will be prescribed a proton pump inhibitor (PPI; rabeprazole or equivalent) to protect your stomach post-operatively
- Sleeve: 1 year
- RYGB: 6 months
- Take this as prescribed
Managing common problems after surgery
| Problem | What to do |
|---|---|
| Constipation | Drink more fluids, stay active, try a stool softener |
| Diarrhea | Stick to clear fluids for 24 hours; avoid sugar-free products with sorbitol |
| Gas and bloating | Walk often; try Gas-X (simethicone) |
| Nausea or vomiting | Sip fluids slowly; don’t eat and drink at the same time; return to liquids if needed |
| Dehydration | Sip fluids all day; watch for dark urine, dizziness, dry mouth |
| Heartburn | Raise the head of the bed; don’t eat before bed; take medications as directed |
⚠ When to call your healthcare team
Contact your surgeon or go to the emergency room if you have:
- Vomiting that lasts more than 24 hours
- Unable to keep any fluids down
- Severe stomach pain
- Fever over 38.5°C (101°F)
- Signs of infection: redness, warmth, or drainage from incisions
- Chest pain or trouble breathing
- Signs of dehydration that do not improve
In an emergency
If you have a medical emergency at any time, call 911 or go to your nearest emergency department.
For Life
Life after surgery
Your lifelong commitments
Bariatric surgery is a powerful tool, but it is not a cure. Long-term success requires your active participation.
1. Take your vitamins every day
Because your body absorbs fewer nutrients after surgery, you must take vitamin and mineral supplements for the rest of your life.
2. Follow nutrition guidelines
- Eat protein first at every meal
- Eat slowly and chew thoroughly
- Stop eating when you feel full
- Do not drink while eating (wait 30 minutes after meals)
- Avoid sugary and high-fat foods
- Stay hydrated – sip fluids throughout the day
The full nutrition guide
For what to eat at each stage — the bariatric plate, protein targets, food lists, sample menus, and recipes — see the companion Nutrition Guide for Bariatric Surgery.
3. Stay physically active
- Aim for 150–300 minutes of activity per week (like brisk walking)
- Include strength training to maintain muscle
- Any activity is better than none – start where you are
4. Attend all follow-up appointments
- Surgeon visit: 4–6 weeks after surgery
- Dietitian: 4 weeks, 8 weeks, 12 weeks, and 6 months post
- Initial lab work: 3 months and 6 months after surgery
- Annual blood work: for the rest of your life
Why follow-up matters
Missing follow-up appointments can lead to serious health problems that develop silently. Nutritional deficiencies can cause nerve damage, bone loss, and other problems if not caught early. Your commitment to lifelong follow-up is as important as the surgery itself.
About weight regain
Some weight regain over time is normal and does not mean you have failed. Reasons for regain can include:
- Your unique genetics and brain biology
- The brain defending against weight loss
- Stomach stretching slightly over years
- Return to old eating habits
- Life stresses, weight-promoting medications, health conditions
If you notice weight regain, do not give up. Talk to your healthcare team. There are options to help:
- Review your eating habits with a dietitian
- Consider adding weight-management medication
- Get support for emotional eating
- In some cases, revision surgery may be an option
Resources & Contacts
Resources and contact information
Western Zone Obesity Network · Website: valleymetabolichealth.com. Here you will find educational resources, support materials, and information about our programs.
Getting a referral
Talk to your family doctor, nurse practitioner, or specialist about getting a referral for bariatric surgery.
Helpful apps
These smartphone apps can help you track food, protein, fluids, and activity:
- Baritastic – designed specifically for bariatric patients
- MyFitnessPal
- Cronometer
Other resources
- Obesity Canada
- Look up the “ASMBS patient video series” on YouTube for education about bariatric surgery
- Nova Scotia Health Wait Times: check current surgical wait times
- Online and local bariatric surgery support groups – ask your healthcare team
You Are Not Alone
You are not alone
Your bariatric surgery journey is about more than weight loss. It is about improving your health, increasing your energy, and enhancing your quality of life.
Success comes from the daily choices you make and the support you accept along the way. Your healthcare team, your family, and your community are here to help you succeed.
Reminders
- Obesity is a medical condition, not a personal failure
- Surgery changes your biology to help you succeed
- Long-term success requires your active participation
- Your healthcare team is here to support you
- Every step forward – no matter how small – is progress
This guide is for educational purposes only and does not replace advice from your healthcare provider. It is based on guidelines from Obesity Canada. Procedure illustrations credited to le Roux et al., “Bariatric Surgery: A Best Practice Article.” Last updated: April 2026.